
On the afternoon of Sunday, 6/30/24, I prelim signed off my last report as a neuroradiology fellow at Yale. It was the last of many lasts. Before fellowship, I remember reading my last case as a resident at Sinai (it was 11 pm Thursday, lol), and I also remember my last sign-out as an internal medicine intern at Greenwich. If counting those six years plus four years of medical school at Cornell, ten long years it’s been since I moved to New York City to begin my medical training. A whole decade. A transformative decade, and it’s just ended!
Continue reading Medical Training Wrap-upCategory Archives: Radiology

2023 in Retrospect
Hi, everyone. This is my blog’s longest running tradition, a yearly wrap-up post.
Continue reading 2023 in Retrospect
End of Residency Email
It’s the end of my radiology residency at Mount Sinai Hospital. I spent my final week reflecting upon my case log from residency, cases mined from four years of dictation, trolling the neuro list, and asking people for fun cases. That’s 1900+ cases of varying educational value, personal significance, or pure visual spectacle. Here are some highlights:
Continue reading End of Residency Email
2022 in Retrospect
2022 was wild. For me, it was filled with big changes, some surprises, and a fair share of challenges. Let’s start with the good news first.
Continue reading 2022 in Retrospect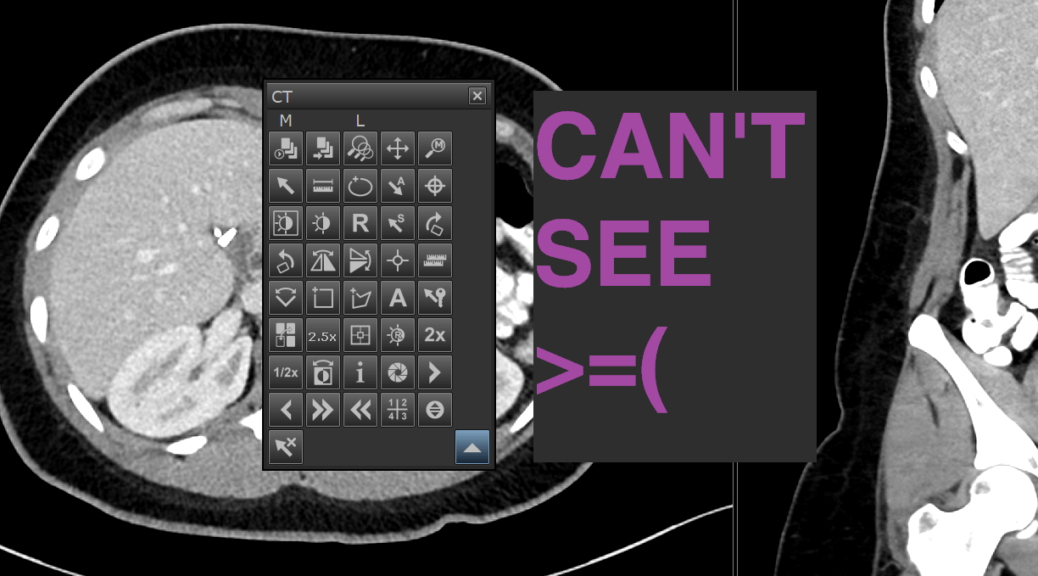
Radiology Workflow Shortcuts
Modern radiology practice is one of high-volume, high-precision visual inspection. Our moment-to-moment visual attention is our singularly essential sensory resource, and we should design our workflow to conserve it. Visual distractions, no matter how brief, should be minimized. Push notifications, invocations of popup menus, glances down at the keyboard, saccades up to a toolbar, and even visually localizing the text cursor in a report all should be avoided.
Example: we have to switch our primary click tool constantly, say from a selection cursor to a 3D-localizing homing tool. I’ve witnessed one of our venerable attendings accomplish this by the following: right click to invoke the tool palette, pause, mouse toward the tool palette expansion command, click, pause, mouse toward the 3D localizer tool, click, mouse toward the X button to close the tool palette, click; then left click to actually use the 3D localizer; and then once again right click, pause, click on the default tool, then click on the X. A tedious and distracting six-second side quest that could be executed with keyboard shortcuts in a near-instantaneous sequence of keystroke, click, keystroke.
Continue reading Radiology Workflow Shortcuts
2021 in Retrospect
Coronavirus, year 2. We’re ending on a sour note, in contrast to the burgeoning promise from last year’s end. I got my first Moderna vaccine dose on 12/31/20 and with it the hope we’d never see a crushing spike in cases again. Depressing that this is the new normal, huh? That this blasted virus can roll around and just ruin plans over and over again. I especially feel for my emergency medicine, internal medicine, and family medicine colleagues who continue to bear the burden of the pandemic on behalf of all of us. Not just in the realm of the hospital, but on behalf of the country as a whole. Thanks, guys.
All right, here’s my annual habit of public reflections. Not much to say.
Radiology
Firstly, I officially declare my radiology class the best class.
Continue reading 2021 in Retrospect
The Toll of Radiology Nights
Radiology night shifts are a frenzy. Maddenly, absurdly difficult. An older internal medicine doctor once asked me “oh, do you get to sleep during your call shifts?” and I scoffed. Sleep?! We hardly have time to go to the bathroom!
Labeling radiology nights as “call” is misleading, suggesting that we only spring into action when some rare clinical circumstance occurs (like checking if a baby’s bowel is twisting itself off). “Night float” gets closer, implying a skeleton night crew takes over to cover overnight emergency issues (like if a patient in the scanner requires special attention). I mean, we do those things too, but the commodity of modern radiology is incorporated real-time into many diagnostic workups, so we’re basically ALWAYS needed.
Continue reading The Toll of Radiology Nights
2020 Personal Review
Originally I had planned but one post to transition from national to personal matters, but once the other post surpassed 3000 words I couldn’t shoehorn this in anymore. So, for my now annual tradition, a self-centric recap:
Continue reading 2020 Personal Review